
Today’s statistics about a sharp rise in paupers’ funerals in the UK provides a stark reminder that more of us are now dying alone, with the number in the south-east of England rising by an astonishing 24 percent in the last year. Loneliness in the UK is at epidemic proportions, so is it now time to rethink what we as communities can do about it?
The links between loneliness and negative health and wellbeing outcomes are impossible to ignore. Research suggests that loneliness is as bad for one’s health as smoking fifteen cigarettes a day and moderate alcohol abuse, and has twice the impact of obesity in causing premature death. As such, loneliness is a clear public health problem and alleviating it through promoting opportunities to form social connections in communities could well generate great benefits in terms of health and wellbeing.
Loneliness manifests in many forms. Bruce Alexander’s theory of dislocation suggests that society in general has become more susceptible to addiction as a result of increased isolation and the fragmentation of families and communities – a negative spiral that can only be remedied through deep changes in the status quo of modern society. Earlier this year Jeremy Hunt said of those who received a pauper’s funeral: “Are we really saying these people had no living relatives or friends? Or is it something sadder, namely that the busy, atomised lives we increasingly lead mean that too often we have become so distant from blood relatives that we don't have any idea even when they are dying? Yes, the health and social care system must do a much better job at looking after them. But so too must all of us as citizens as well.”
In an economic and political climate where there is renewed interest in the role of the citizen, we are being asked to think deeply about our own role in our own communities. This began with “the Big Society” rhetoric in 2010, but it remains a key theme across public service providers, with high profile calls for citizen empowerment such as 2014’s NHS Five Year Forward View which highlighted the importance of the National Health Service drawing on the ‘renewable energy presented by patients and communities’.
Seeding a social movement for health
But to encourage citizen action for health, we might need to radically change the way we understand what public health is. This requires a move beyond the traditional, top-down, evidence-based health paradigm to one that places social connectedness at the heart of health and wellbeing. To really embrace this requires a kind of shift that will take the certainty out of delivery and raise very real concerns about safeguarding and risk for those tasked with commissioning services. But if the active citizen is really to play a role, then services must be able to empower and harness the latent energy of individuals and their social networks – handing over the metaphorical keys and putting the citizen in the driving seat. By enhancing capacity for, and confidence in, people’s sense of agency, only then will we create the conditions for more socially productive citizens and services.
In recent years the concept of coproduction and asset-based community development has gained real traction in public services. This focuses attention not on a community’s needs and deficits, but on its skills and capabilities. Its rapid adoption is symptomatic of a new trend towards a less patrician form of public service management. These approaches aim to build community capacities to take action on health and the social determinants of health, bringing people together to determine what they themselves can do to support their own health and wellbeing.
Connecting communities through coproduction
Since 2010 the RSA and its partners at the University of Central Lancashire (UCLan) and the London School of Economics (LSE) have been testing coproduction methods and their efficacy as tools to tackle social isolation and improve community wellbeing in a five year Big Lottery Funded programme. Working with communities in seven locations in England to research and strengthen relationships within communities, we applied the below model of change.
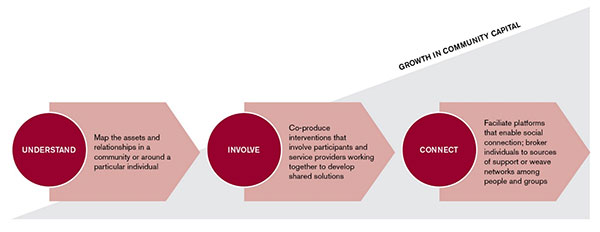
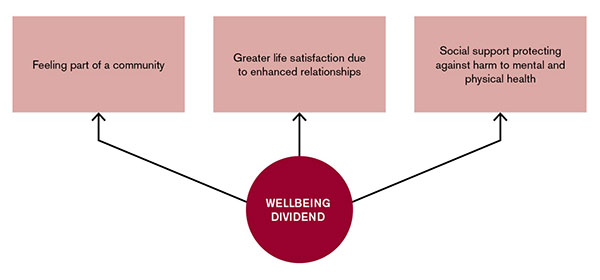
The vision of our ‘Connected Communities’ programme is one in which people are embedded within local networks of social support; where social isolation is reduced, and people experience greater wellbeing and other benefits from the better understanding, mobilisation and growth of ‘community capital’ in their neighbourhoods. Expanding on the thinking of Putnam and Bourdieu, we developed the term ‘community capital’, which means the sum of assets and benefits derived from the relationships within a community. To tackle a rising tide of loneliness, we advocate that efforts to grow community capital be made a priority by health and social care commissioners. By strengthening and connecting communities, our research was able to demonstrate (in a small cohort) that a wellbeing dividend from social connectedness might mitigate against mental and physical ill health in the longer term – supporting the case for investing in efforts to make communities more socially connected.
Beyond loneliness, coproduction models are making inroads in services for communities and individuals with more complex needs. In our Whole Person Recovery programme, our research into “recovery capital” is demonstrating that recovery is not just or always about the absence of something (for example, drugs or alcohol) but the presence of other things such as social networks, meaningful work and access to adequate housing and financial resources. These other things are inherently difficult to measure, but by combining individuals into a group that can create networked support and coproduce services, their capability can become greater. In simple terms, a community’s power to create positive change is greater than an individual’s.
A movement for change?
While there is now widespread adoption of the concept of coproduction – delivery is still patchy across the country and there is some need for commissioners to ‘catch up’ with the evidence and the sea change in approaches that are taking place in many areas (such as Essex as and Kent). To drive a social movement for health will mean reconnecting and supporting innovation on the ground, particularly in relation to the role of peers and local communities in supporting themselves locally. There is also a need to develop a national evidence base for community-driven health. The Institute for Health and Wellbeing at Leeds Beckett has been building such an evidence base led by the work of Professor Jane South. Working with Public Health England, she recently launched a guide to community-centred approaches to health and wellbeing which outlines a ‘family of approaches’ for evidence-based community-centred approaches for health and wellbeing.
But research evidence alone will not be enough – a social movement can only be led by people. If the aim is to see profound system change, then we must now take the public debate a step further and engage with people and communities in a dialogue about the social determinants of health and wellbeing, the systemic challenges in the current, often atomised model of care, and the opportunities of a new approach where ‘public’ health is our health ‘system’. A system where public services are inherently people services.
Tonight at the RSA we will be hosting a seminar on Communities Creating Health to kick start this debate – we hope you can join us online.
Follow me on @rowaneconway
Join the discussion
Comments
Please login to post a comment or reply
Don't have an account? Click here to register.
This all makes perfect sense, but the emphasis on community engagement and support is not new. Tme Banking, which is based on co-production, has been active in the UK for many years - the idea was first developed by Edgar Kahn in the US who received an Ashoka Fellowship for it - and there are now hundreds of them across the UK.
Time banks are open to all but are particularly helpful for people who are unable to take part in mainstream life, whether because of poverty, disability, mental health issues or isolation due to language barriers, or just being new to an area. As well as building individual well-being, they help strengthen communities, building friendships, and giving a sense of identity.
Your research should help by convincing local authorities and CCGs to fund them, thereby saving the NHS and social services considerable sums as people become happier, healthier and more able to cope.